Question: I am not inclined to take supplements (e.g. stimulants) to lose weight, but I can’t seem to stay with any program long enough to reach my goal weight. Can supplements help?
Answer: Yes, because as you said, you can’t seem to stick to a program. But you knew we would say that because we sell supplements. Both supplements and meal replacement bars and drinks can help you reach your goal. Diet drugs or supplements are incorporated into a weight loss program to assist the participant in complying with a daily routine that leads to weight reduction. In other words, to make it easier to control appetite and burn calories until you feel you have your daily routine under control. At that point you should be able to continue making progress without the supplements (which means burning more calories than you consume). Once you reach the weight or body composition goal, there is no longer a need to burn more calories than you consume. You can now increase your caloric intake to a maintenance level (consume as much as you burn), which should also help relieve the need for supplementation (read "Use of Supplements for Fat Loss", the complete dotFIT position on the use of dietary supplements in support of body fat/weight loss).
More info
There are dietary supplements that have shown great promise in assisting weight loss by helping control appetite through inducing feelings of fullness sooner and longer and blocking calorie absorption, which allows the user the act and satisfaction of eating while reducing the body’s calorie uptake. Additionally, many dietary supplements can naturally increase the user’s ability to burn calories, making it easier to continue to lose fat (get more info on dotFIT products featuring ingredients shown to enhance fat loss: FatRelease, CarbRepel, ThermAccel.
Meal replacements
Although standard meal replacements (MR) are not considered supplements since they are actually food, our first recommendation in support of weight loss is to incorporate one or two meal replacement bars or drinks into your daily diet, allowing greater freedom of choice for your remaining calories.
Here’s why
In all studies, meal replacements have been shown to be an extremely effective aid to weight reduction and, in almost all cases, more effective than conventional methods of dietary restrictions (see Figure 1). Additionally, meal replacements have been shown to be just as effective as dietary restriction combined with pharmacological therapy. And most importantly, continuous use of meal replacements may be the most effective means of all treatments when it comes to maintaining weight loss (see Figure 2).
Meal replacements are generally used to replace one or two meals a day and allow freedom of choice for the remaining allotted foods/calories.
Meal replacements allow:
- Portion control: people generally attempt to consume meals to completion, , therefore meal portion size significantly impacts a person’s total calorie intake. Overwhelming evidence validates that the smaller the portions, the fewer daily calories consumed and vice-versa – i.e. people tend to “eat with their eyes not their stomachs”. Use of portion-controlled meals has proven to yield greater weight loss than conventional diet therapy alone.
- Accurate calorie counts of total daily food intake when compared to having to estimate the calories of self-prepared or unmarked meals.
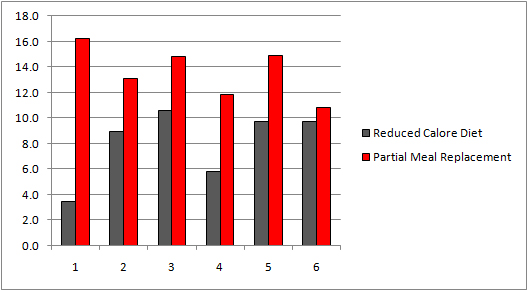 Figure 1:
Figure 1: In all six studies the groups using meal replacements (PMR) as part of their overall calorie intake lost significantly more weight than subjects using the reduced calorie diet (RCD) alone. Heymsfield SB (2003)
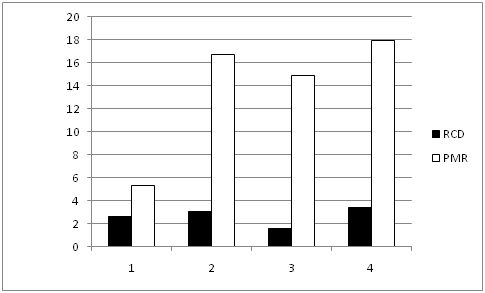 Figure 2:
Figure 2: In a 1-year follow-up in the groups that were tracked, the subjects still using meal replacements (PMR) maintained significantly more weight loss than the RCD group. Heymsfield SB (2003)
References
- Heymsfield SB, van Mierlo CA, van der Knaap HC, Heo M, Frier HI. Weight management using a meal replacement strategy: meta and pooling analysis from six studies. Int J Obes Relat Metab Disord. 2003 May;27(5):537-49.
- Ashley JM, St Jeor ST, Perumean-Chaney S, Schrage J, Bovee V. Meal replacements in weight intervention. Obes Res. 2001 Nov;9 Suppl 4:312S-320S.
- Ditschuneit HH. Do meal replacement drinks have a role in diabetes management? Nestle Nutr Workshop Ser Clin Perform Programme. 2006;11:171-9; discussion 179-81. Review.
- Li Z, Hong K, Saltsman P, DeShields S, Bellman M, Thames G, Liu Y, Wang HJ, Elashoff R, Heber D. Long-term efficacy of soy-based meal replacements vs an individualized diet plan in obese type II DM patients: relative effects on weight loss, metabolic parameters, and C-reactive protein. Eur J Clin Nutr. 2005 Mar;59(3):411-8.
- Poston WS, Haddock CK, Pinkston MM, Pace P, Karakoc ND, Reeves RS, Foreyt JP. Weight loss with meal replacement and meal replacement plus snacks: a randomized trial. Int J Obes (Lond). 2005 Sep;29(9):1107-14.
- Douketis JD, Macie C, Thabane L, Williamson DF. Systematic review of long-term weight loss studies in obese adults: clinical significance and applicability to clinical practice. Int J Obes (Lond). 2005 Oct;29(10):1153-67. Review.
- Ditschuneit HH, Flechtner-Mors M. Value of structured meals for weight management: risk factors and long-term weight maintenance. Obes Res. 2001 Nov;9 Suppl 4:284S-289S.
- Rothacker DQ. Five-year self-management of weight using meal replacements: comparison with matched controls in rural Wisconsin. Nutrition 2000;16:344–8.
- Flechtner-Mors M, Ditschuneit HH, Johnson TD, Suchard MA, Adler G. Metabolic and weight loss effects of long-term dietary intervention in obese patients: four-year results. Obes Res. 2000 Aug;8(5):399-402.
- McGuire MT, Wing RR, Klem ML, Lang W, Hill JO. What predicts weight regain in a group of successful weight losers? J Consult Clin Psychol 1999;67:177–85.
- Levitsky DA, Youn T. The more food young adults are served, the more they overeat. J Nutr. 2004 Oct;134(10):2546-9.
- Wansink B, Painter JE, North J. Bottomless bowls: why visual cues of portion size may influence intake. Obes Res. 2005 Jan;13(1):93-100.
- Rolls BJ, Roe LS, Meengs JS. Reductions in portion size and energy density of foods are additive and lead to sustained decreases in energy intake. Am J Clin Nutr. 2006 Jan;83(1):11-7.
- Zheng G, Sayama K, Okubo T, Juneja LR, Oguni I. Anti-obesity effects of three major components of green tea, catechins, caffeine and theanine, in mice. In Vivo. 2004 Jan-Feb;18(1):55-62.
- Tappenden KA, Martin A, Layman DK, Baum J. Evaluation of the efficacy of an amylase inhibitor. FASEB 2001; 15(4):A301.
- Jeffery RW, Wing RR, Thorson C, Burton LR, Raether C, Harvey J, Mullen M. Strengthening behavioral interventions for weight loss: a randomized trial of food provision and monetary incentives. J Consult Clin Psychol. 1993 Dec;61(6):1038-45
- McCarron DA, Oparil S, Chait A, Haynes RB, Kris-Etherton P, Stern JS, Resnick LM, Clark S, Morris CD, Hatton DC, Metz JA, McMahon M, Holcomb S, Snyder GW, Pi-Sunyer FX. Nutritional management of cardiovascular risk factors. A randomized clinical trial. Arch Intern Med. 1997 Jan 27;157(2):169-77.
- Wing RR, Jeffery RW. Food provision as a strategy to promote weight loss. Obes Res. 2001 Nov;9 Suppl 4:271S-275S. Review.
- Wing RR, Jeffery RW, Burton LR, Thorson C, Nissinoff KS, Baxter JE. Food provision vs structured meal plans in the behavioral treatment of obesity. Int J Obes Relat Metab Disord. 1996 Jan;20(1):56-62.
- Abbot JM, Thomson CA, Ranger-Moore J, Teixeira PJ, Lohman TG, Taren DL, Cussler E, Going SB, Houtkooper LB. Psychosocial and behavioral profile and predictors of self-reported energy underreporting in obese middle-aged women. J Am Diet Assoc. 2008 Jan;108(1):114-9.